

Benjamin Wolfe, Tufts University
When you hear about the gut microbiome, does it ever make you wonder what tiny creatures are teeming inside your own body? As a microbiologist who studies the microbiomes of plants, animals and people, I’ve watched public interest in gut microbes grow alongside research on their possible dramatic influence on human health. In the past several years, microbiome testing techniques used by researchers like me are now available to consumers at home. These personal gut microbiome testing kits claim to tell you what organisms live in your gut and how to improve your gut microbiome using that data.
I became very interested in how these home test kits work, what kind of information they provide and whether they can really help you change your gut microbiome. So I ordered a few kits from Viome, Biohm and Floré, tried them out and sifted through my own microbiome data. Here is what I learned. https://www.youtube.com/embed/VzPD009qTN4?wmode=transparent&start=0 Your gut microbiome can be a partner in your health – if you have the right bacteria.
How do gut microbiome kits work?
All gut microbiome kits require you to carefully collect fresh fecal material. You put it in the various tubes provided in the kit and mail the samples back to the company. Several weeks later, you’ll receive a report describing the types of microbes living in your gut and suggestions on how to change your diet or activities to potentially alter your gut microbiome.
What consumers don’t exactly know is how companies generate the microbial profile data from your fecal sample. A typical approach I and other microbiome researchers use is to extract and decode the microbial genetic material from a sample. We use that genetic material to identify what species of microbes are present. The challenge is that this process can be done in many different ways, and there are no widely agreed-upon standards for what is the best method.

For example, microbiome analyses can be done on two types of genetic material, RNA or DNA. If the profile is based on DNA, it can give you a snapshot only of what types of microbes are present, not what microbial genes are active or what activities they are doing in your body. On the other hand, if the profile is based on RNA, it can tell you not only what microbes are present, but also whether they’re playing a role in your digestion or producing metabolites that can reduce gut inflammation, among other functions. Viome generates its profiles by looking at RNA, while the other companies use DNA.
Other data analysis choices, such as how different types of genetic sequences are sorted or which databases are used to identify the microbes, can also affect the level of detail and utility of the final data. Microbiome scientists are usually very careful to point out these nuances when interpreting their own data in scientific papers, but these details are not clearly presented in home microbiome kits.
What I learned about my gut microbiome
Though I used the same fecal sample for each kit, mixed well to ensure uniformity, I was surprised that each of the three products I tried gave me different impressions of my gut microbiome.
Each company gives an overall “score” on how your microbiome compares with what they consider to be “good” or “healthy.” My scores ranged from 39% (not great) to 72% (good). Interestingly, Viome, which infers microbial activity by using RNA, gave the lowest score. It noted that certain microbial activities happening in my gut, such as methane production and digestion efficiency, were not optimal.
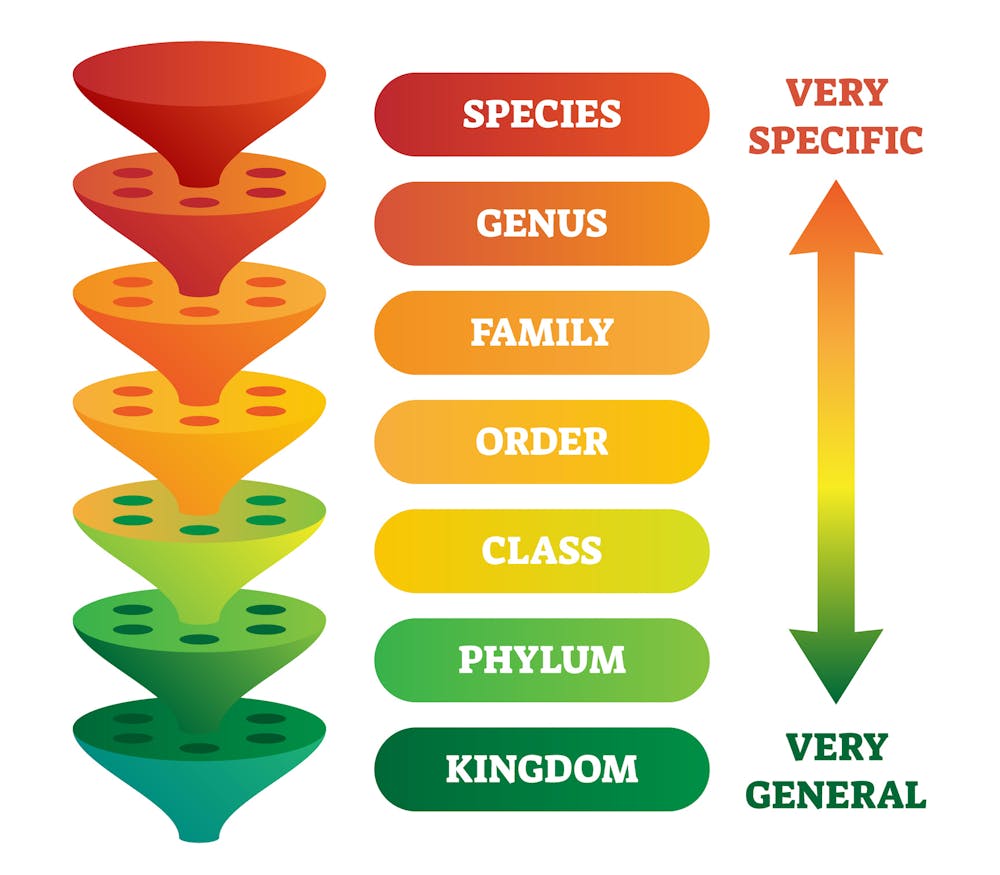
I was also surprised by the variation in total microbial diversity each company reported. While there was general agreement in the overall groups of microbes present at the phylum level, a more general biological grouping, there was a huge range of variation at the species level, the most specific grouping. One company reported 527 species of microbes in my microbiome, while another reported 312. One reported only 27.
Perhaps the most surprising most surprising finding was that my gut may harbor a microbe that could (there are many caveats here!) pose a problem for me in the future if I experience certain medical situations. Even though all companies explicitly looked for this microbe in my gut microbiome sample, only two actually found it. While I won’t name the exact microbe to protect my health privacy, I am not too worried about this result because more information, such as full genome sequencing of the microbe, is needed to better understand if this is actually a concerning strain of this microbe. But this finding does point to some surprising variation in results across different testing kits.
Can this data really improve your gut microbiome?
Many microbiome scientists like me would probably argue that the data these kits provide are limited in terms of giving you the power to alter your health. This is partly because gut microbiome science is still a new field with many unanswered questions.
One challenge is that different people can have different proportions of microbes present in their gut. This variation has made it difficult for scientists and health professionals to agree on what type of microbial community makes a gut “healthy.” Some specific species, such as the bacterium C. diff, and some broad groups, like Proteobacteria, are usually considered undesirable in high amounts. But there is no clear consensus on why one microbiome might be better than another.
Even if you did try to improve your gut microbiome based on what your gut test told you, the results might not turn out as you hoped. Probiotics or diet changes can alter the diversity of your gut microbiome and how it functions, but studies often find that each person can have different responses to these interventions, possibly because of their own unique microbiome composition. The personalized ecology of gut microbial communities, combined with genetics, diet and other factors, makes it challenging to prescribe universal solutions.
So why bother getting a gut microbiome test? For me, it was illuminating to learn what microbes I carry around with me each day. When I eat my lunch, go for a run or get stressed out, the microbes in my gut respond to changes in my body. Researchers may not completely understand what those changes mean and how to manage our microbial partners, but getting to know who they are is a great first step.
Benjamin Wolfe, Associate Professor of Biology, Tufts University
This article is republished from The Conversation under a Creative Commons license. Read the original article.













 (
( – As mayor of D’Lo, Mississippi, one of John Henry Berry’s recent challenges included tracking down errant employees — goats he had positioned to clip the town’s ball fields had wandered off. The quest for the goats is an example of the quirky challenges facing Mayor Berry and featured in the reality series, “Small Town, Big Mayor,” airing on UP TV on Thursdays at 9:30 p.m. Eastern time.The series offers a refreshing escape from the negative attitude surrounding much of politics today with a behind-the-scenes look at a hard-working mayor and his family who want to make their town a better place and to help it survive and thrive in the future.The residents of D’Lo include 456 people, as well as 240 cows. Mayor Berry wears multiple hats, serving not only as mayor, but also as town arbitrator, dog catcher, landscaper, sewer repairman, volunteer fireman, high school football announcer, Parish drummer, and 4H Firearms Instructor, to name a few. He also finds time to be the father of five children: Ashley, Ben, Autumn, Preston, and Josh; and husband to Angie.The fourth-generation resident of D’Lo is known for his positive attitude, white suits, and the inclination to drive around town in a golf cart.”The love of my town inspired me to run for mayor,” says Mayor Berry. “As a native of D’Lo, Miss., I want to improve the town and bring in tourism,” he adds. Specific plans to attract tourists include opening a restaurant, he notes.In addition to the restaurant, his goals include legalizing golf carts in D’Lo, making the town more environmentally friendly, putting D’Lo on Kickstarter, building a library, and launching a campaign to recruit new volunteer firemen.Each episode of “Small Town, Big Mayor” will focus on some aspect of his 95-point plan to revitalize the town.In the meantime, Mayor Berry gracefully juggles daily challenges of small-town administrations.”There’s nothing I won’t do for D’Lo,” says Berry. One surprise: “I had to learn to work on the water well and sewage system to keep things functioning properly without spending money the city didn’t have,” he says.Tune in to “Small Town, Big Mayor” for a taste of genuine community spirit as the citizens rally around the mayor. As Mayor Berry says, “We may be tiny, but we have a lot of heart.”
– As mayor of D’Lo, Mississippi, one of John Henry Berry’s recent challenges included tracking down errant employees — goats he had positioned to clip the town’s ball fields had wandered off. The quest for the goats is an example of the quirky challenges facing Mayor Berry and featured in the reality series, “Small Town, Big Mayor,” airing on UP TV on Thursdays at 9:30 p.m. Eastern time.The series offers a refreshing escape from the negative attitude surrounding much of politics today with a behind-the-scenes look at a hard-working mayor and his family who want to make their town a better place and to help it survive and thrive in the future.The residents of D’Lo include 456 people, as well as 240 cows. Mayor Berry wears multiple hats, serving not only as mayor, but also as town arbitrator, dog catcher, landscaper, sewer repairman, volunteer fireman, high school football announcer, Parish drummer, and 4H Firearms Instructor, to name a few. He also finds time to be the father of five children: Ashley, Ben, Autumn, Preston, and Josh; and husband to Angie.The fourth-generation resident of D’Lo is known for his positive attitude, white suits, and the inclination to drive around town in a golf cart.”The love of my town inspired me to run for mayor,” says Mayor Berry. “As a native of D’Lo, Miss., I want to improve the town and bring in tourism,” he adds. Specific plans to attract tourists include opening a restaurant, he notes.In addition to the restaurant, his goals include legalizing golf carts in D’Lo, making the town more environmentally friendly, putting D’Lo on Kickstarter, building a library, and launching a campaign to recruit new volunteer firemen.Each episode of “Small Town, Big Mayor” will focus on some aspect of his 95-point plan to revitalize the town.In the meantime, Mayor Berry gracefully juggles daily challenges of small-town administrations.”There’s nothing I won’t do for D’Lo,” says Berry. One surprise: “I had to learn to work on the water well and sewage system to keep things functioning properly without spending money the city didn’t have,” he says.Tune in to “Small Town, Big Mayor” for a taste of genuine community spirit as the citizens rally around the mayor. As Mayor Berry says, “We may be tiny, but we have a lot of heart.”
 (
( – -In the wake of the ongoing pandemic, many people have taken the opportunity for introspection, and many are exploring spirituality and the meaning of the universe in a new way.For Christians, God is the creator, and a new book explores a unique way of examining creation from the perspective of quantum physics, and the interaction of music, light, and sound.Len Mink, a show business veteran, discovered his personal relationship with Jesus in 1971, a relationship that sustained him through a bout with a potentially terminal blood disease. However, he was cured and continued his work as a composer and performer.Mink has produced more than 30 albums of contemporary Christian music as well as hymns projects.Most recently, Mink channeled his musical background to delve into the relationship between music, science, and the realm of the Spirit.In his book, “The Supernatural Power of Music — A Quantum Leap Into Worship,” he presents the essence of the connection among sound, light, music, worship, and quantum physics.”It seems that ‘quantum speak’ and ‘faith speak’ are one and the same,” says Mink.”Science is the discipline of discovering things that already exist,” he adds. Mr. Mink takes readers on a journey into the musicality of the universe, from quasars to crickets.The relationship between music and quantum physics continues to be an area of intrigue and study.A recent article on the PBS website’s NOVA section notes that, in fact, the universe is built on harmonies, and that mathematical patterns not only define musical scales that make the tunes we love to hear, they also describe the waves and frequencies involved in quantum physics and studied by scientists over the ages.”The well-known phrase, ‘knowledge is power,’ is visibly demonstrated in this treasure chest of revelation, giving us an exciting look into both the macro and micro-universe,” Mink notes.Mink’s goal in writing the book is to awaken the spiritual in all people, breathe divine energy into every level of one’s being, and “unlock the life that your heart has been desperately hungering for,” he says.”We live in an ever-revealing cosmos, teeming with the frequencies of life, bombarding you and affecting your emotions, your moods, your mind, and even your physical body. Open your whole being to the Divine Orchestrator and experience the ‘Supernatural Power of Music,’Mink urges.The book is available in paperback direct from Len Mink Ministries or Amazon, through download on Kindle, and audiobook in MP3 and CD format (read by author).For more information, visit lenandcathymink.org.
– -In the wake of the ongoing pandemic, many people have taken the opportunity for introspection, and many are exploring spirituality and the meaning of the universe in a new way.For Christians, God is the creator, and a new book explores a unique way of examining creation from the perspective of quantum physics, and the interaction of music, light, and sound.Len Mink, a show business veteran, discovered his personal relationship with Jesus in 1971, a relationship that sustained him through a bout with a potentially terminal blood disease. However, he was cured and continued his work as a composer and performer.Mink has produced more than 30 albums of contemporary Christian music as well as hymns projects.Most recently, Mink channeled his musical background to delve into the relationship between music, science, and the realm of the Spirit.In his book, “The Supernatural Power of Music — A Quantum Leap Into Worship,” he presents the essence of the connection among sound, light, music, worship, and quantum physics.”It seems that ‘quantum speak’ and ‘faith speak’ are one and the same,” says Mink.”Science is the discipline of discovering things that already exist,” he adds. Mr. Mink takes readers on a journey into the musicality of the universe, from quasars to crickets.The relationship between music and quantum physics continues to be an area of intrigue and study.A recent article on the PBS website’s NOVA section notes that, in fact, the universe is built on harmonies, and that mathematical patterns not only define musical scales that make the tunes we love to hear, they also describe the waves and frequencies involved in quantum physics and studied by scientists over the ages.”The well-known phrase, ‘knowledge is power,’ is visibly demonstrated in this treasure chest of revelation, giving us an exciting look into both the macro and micro-universe,” Mink notes.Mink’s goal in writing the book is to awaken the spiritual in all people, breathe divine energy into every level of one’s being, and “unlock the life that your heart has been desperately hungering for,” he says.”We live in an ever-revealing cosmos, teeming with the frequencies of life, bombarding you and affecting your emotions, your moods, your mind, and even your physical body. Open your whole being to the Divine Orchestrator and experience the ‘Supernatural Power of Music,’Mink urges.The book is available in paperback direct from Len Mink Ministries or Amazon, through download on Kindle, and audiobook in MP3 and CD format (read by author).For more information, visit lenandcathymink.org.
 (
( -Approximately half of U.S. adults have high blood pressure, but many don’t know it, according to the American Heart Association. A new public service campaign from the American Heart Association, American Medical Association and Ad Council in partnership with HHS Office of Minority Health and Health Resources & Services Administration encourages all adults to take control by monitoring their blood pressure at home and sharing the numbers with their doctor.The “Get Down with Your Blood Pressure” public service announcement uses catchy music and memorable dance moves to get the attention of people who have and are at increased risk for high blood pressure and negative health consequences associated with it, such as heart attack, stroke and severe complications of COVID-19.The campaign keeps it simple, and encourages those with high blood pressure to regularly follow four easy steps: “Get It, Slip It, Cuff It, Check It.” That means Get the blood pressure cuff, Slip it on, use the band to Cuff your arm, Check your blood pressure with a validated monitor and share the numbers with your doctor. The campaign’s detailed instructional videos are available in English and Spanish.”This new campaign is a fun way to get people engaged in monitoring their blood pressure and keeping it under control — which can often feel daunting to many patients”– and is timely given that high blood pressure puts patients at higher risk of severe complications of COVID-19,” says American Medical Association president Gerald E. Harmon, M.D. “We are committed to eliminating structural drivers of health inequities that place Black and Brown communities at increasing risk of heart disease,” Dr. Harmon adds.The campaign emphasizes self-monitoring and encourages individuals to work with their doctors to create a personalized plan to manage and treat high blood pressure. Changes to unhealthy eating habits and increases in physical activity may be all it takes to get your blood pressure to a healthy range. However, sometimes it’s not that simple. If your doctor prescribes a blood pressure medication, be sure to take it as directed.”This campaign is part of the American Heart Association’s National Hypertension Control Initiative,” says Donald M. Lloyd-Jones, M.D., ScM, F.A.H.A., president of the American Heart Association, chair of the Department of Preventive Medicine and Eileen M. Foell Professor of Heart Research and Professor of Preventive Medicine, Medicine, and Pediatrics at Northwestern University Feinberg School of Medicine in Chicago, Illinois. “The initiative encompasses direct education and training on blood pressure measurement and management with health care professionals in community health centers and community-based organizations. We are meeting people where they are with access to blood pressure education and resources to reduce high blood pressure in communities that need it most.”Visit
-Approximately half of U.S. adults have high blood pressure, but many don’t know it, according to the American Heart Association. A new public service campaign from the American Heart Association, American Medical Association and Ad Council in partnership with HHS Office of Minority Health and Health Resources & Services Administration encourages all adults to take control by monitoring their blood pressure at home and sharing the numbers with their doctor.The “Get Down with Your Blood Pressure” public service announcement uses catchy music and memorable dance moves to get the attention of people who have and are at increased risk for high blood pressure and negative health consequences associated with it, such as heart attack, stroke and severe complications of COVID-19.The campaign keeps it simple, and encourages those with high blood pressure to regularly follow four easy steps: “Get It, Slip It, Cuff It, Check It.” That means Get the blood pressure cuff, Slip it on, use the band to Cuff your arm, Check your blood pressure with a validated monitor and share the numbers with your doctor. The campaign’s detailed instructional videos are available in English and Spanish.”This new campaign is a fun way to get people engaged in monitoring their blood pressure and keeping it under control — which can often feel daunting to many patients”– and is timely given that high blood pressure puts patients at higher risk of severe complications of COVID-19,” says American Medical Association president Gerald E. Harmon, M.D. “We are committed to eliminating structural drivers of health inequities that place Black and Brown communities at increasing risk of heart disease,” Dr. Harmon adds.The campaign emphasizes self-monitoring and encourages individuals to work with their doctors to create a personalized plan to manage and treat high blood pressure. Changes to unhealthy eating habits and increases in physical activity may be all it takes to get your blood pressure to a healthy range. However, sometimes it’s not that simple. If your doctor prescribes a blood pressure medication, be sure to take it as directed.”This campaign is part of the American Heart Association’s National Hypertension Control Initiative,” says Donald M. Lloyd-Jones, M.D., ScM, F.A.H.A., president of the American Heart Association, chair of the Department of Preventive Medicine and Eileen M. Foell Professor of Heart Research and Professor of Preventive Medicine, Medicine, and Pediatrics at Northwestern University Feinberg School of Medicine in Chicago, Illinois. “The initiative encompasses direct education and training on blood pressure measurement and management with health care professionals in community health centers and community-based organizations. We are meeting people where they are with access to blood pressure education and resources to reduce high blood pressure in communities that need it most.”Visit 
 (
( – Who hasn’t heard of the “Freshman 15”? According to Nick Rizzo at
– Who hasn’t heard of the “Freshman 15”? According to Nick Rizzo at 
 (
( – Making healthy food choices can be overwhelming, especially if money is tight. Good nutrition is at the core of good health and reducing risk of cardiovascular disease, such as heart disease and stroke. “Eating delicious nourishing meals on a budget is possible, especially with a few key tips to make it simple,” says Bridget Wojciak, director of nutrition and dietetics at Kroger Health, a national sponsor of the American Heart Association’s Healthy for Good initiative. Planning ahead can help your dollar go further.The American Heart Association has developed tips to help families shop, eat and cook healthier meals on a budget.
– Making healthy food choices can be overwhelming, especially if money is tight. Good nutrition is at the core of good health and reducing risk of cardiovascular disease, such as heart disease and stroke. “Eating delicious nourishing meals on a budget is possible, especially with a few key tips to make it simple,” says Bridget Wojciak, director of nutrition and dietetics at Kroger Health, a national sponsor of the American Heart Association’s Healthy for Good initiative. Planning ahead can help your dollar go further.The American Heart Association has developed tips to help families shop, eat and cook healthier meals on a budget.